


[ad_1]
The call had come in as a 61-year-old male with difficulty breathing. The dispatcher had flagged it as a probable Covid-19 case. A woman wearing scrubs and a face mask peered down from the window at Complete Care nursing home as paramedics Alex Storzillo and Jim Incorvaia entered, wearing respirators that covered their whole face.
Inside, they found the man, who had a fever for several days, and was now barely alert. His oxygen saturation and blood pressure were very low.
He needed to be intubated and rushed to the hospital, where he could be placed on a ventilator.
For Storzillo and Incorvaia and so many paramedic colleagues across the country, this is their new routine, their daily grind: Trying to save lives while risking exposure to Covid-19, the deadly disease caused by coronavirus.
‘No such thing as being more sick than that’

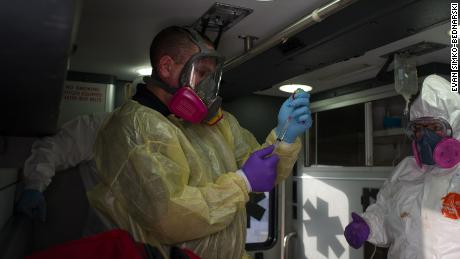
In the ambulance, standing by the man’s feet near the open rear doors, Storzillo, 29, prepared what he’d called “half of a lethal injection,” a combination of sedative and paralytic meant to halt a patient’s breathing so that the paramedics could take over.
Incorvaia, 31, phoned ahead to the emergency room. “He feels very hot,” he said to the doctor on the other end of the line. “We know he has Parkinson’s, he has kidney failure, and he has (a history of) hypertension.”
Back in the ambulance, the man’s blood pressure was so low that Storzillo couldn’t find a vein to administer the drugs. Instead, the paramedics drilled into the man’s shin, allowing Storzillo to inject the medication into the man’s bone marrow.
In about a minute, the man was completely paralyzed.
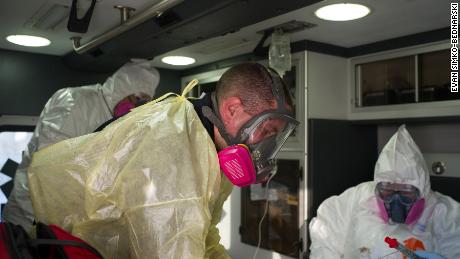
Now up at the man’s head, Incorvaia began to work. Aided by a small video camera placed down the throat, Incorvaia guided a breathing tube through the man’s mouth, past his vocal cords, and into his trachea.

Storzillo came up alongside and attached a tough plastic bladder to the tube, squeezing it rhythmically. He had now taken over the most fundamental of human tasks: breathing.
Sitting at the man’s chest, Nicole Tugwell, an emergency medical technician on loan from Baltimore, took the bag. For the next 10 minutes, as the ambulance headed to the hospital, she would be the man’s lungs.
Storzillo, meanwhile, placed a blood pressure cuff around a bag of saline solution hanging from the ceiling and tied in to the IV. He pumped up the cuff in an effort to squeeze the bag and maintain the patient’s blood pressure.
Later, after delivering the man to the emergency room at St. Joseph’s Regional Medical Center in Paterson, Incorvaia summed up the patient’s condition.
“There really is no such thing as being more sick than that,” he said.
Their bond is forged by ink

Storzillo and Incorvaia have been partners on the streets of Paterson for a little over a year but they’ve been friends since they were teenagers: They met as cadets in the Civil Air Patrol in northern New Jersey.
The pair work for the mobile intensive care unit at St. Joseph’s, serving an emergency room that, by the hospital’s own count, was the third busiest in the nation last year.
An early Wednesday morning last week found them taking inventory of medication and equipment in the back of their truck while an ultraviolet light hung in the cab, decontaminating the vehicle before their 12-hour shift.
As they worked their tattooed forearms were visible, revealing their matching ink: “VERITAS,” Latin for “truth,” below Incorvaia’s left elbow; “AEQUITAS”– “justice”– below Storzillo’s right elbow.
It’s a reference, they said, to the 1999 cult-classic shoot-em-up “The Boondock Saints.”
In the office adjoining the paramedics’ three-bay garage, Storzillo’s black Les Paul guitar sat in its case. In less disease-ridden times, he’d be playing out around north Jersey with his band the Grease Guns.
But these days, as the two friends race around Paterson, bringing urgent life support to ailing residents, Storzillo plays a different instrument.
“I’m like Mozart with the siren,” he joked, while navigating one crowded intersection with a particularly staccato wail from the truck.

Paramedics, distinct from EMTs, are practitioners of what is termed “advanced life support.” They are authorized to give medications and perform high-risk and invasive procedures, and are often the highest medical authority on-scene.
“We get dispatched to more higher acuity emergencies — shortness of breath, diabetic emergencies, seizures, chest pain, things like that,” Storzillo said.
“Right now,” he continued, “we’re almost getting dispatched for exclusively respiratory calls.”
For a disease that targets the lungs, radio calls for “respiratory problems” have become the pandemic’s refrain.
While EMTs head to a call in an ambulance, the paramedics of Paterson meet them for the most difficult jobs. The back of their truck is stocked with medication, specialized equipment, and a combination heart-monitor/defibrillator/external-pacemaker called a Lifepak.
“We can get in there and we can intervene early,” Storzillo said, “and hopefully set these patients up for a better outcome down the line.”
They take ‘a very high risk’ to save lives
Under ordinary circumstances, an in-the-field intubation using paralytic drugs — known as a rapid-sequence intubation — is a risky procedure for them and for the patient. In the time of Covid-19, a procedure like the one Storzillo and Incorvaia performed outside the nursing home is downright dangerous.
“It’s the most high-risk procedure we can do in this job,” Incorvaia said later. “We’re taking someone who’s able to breathe on their own, we’re sedating them, we’re paralyzing them, and we’re taking that ability for them to breathe away.”
Intubation, as the medics put it, serves to “manage” a patient’s airway — to get them breathing as consistently functionally as possible when there is reason to believe that they can’t do that alone. Those reasons can be as varied as an acute lung infection like Covid-19, heart failure, or head trauma.

And when the decision is made to intubate, the paramedics need to ensure that the patient doesn’t try to fight the new breathing rhythm with their own lungs, or try to remove the tube that’s been carefully threaded down their throat, through their vocal cords, and into their trachea.
“It’s a lot of liability, it’s a lot of stress, and it could go south if done incorrectly,” Incorvaia said.
Before Covid-19, such field intubations were not terribly common. But now, in the midst of a pandemic, the paramedics said they are doing them more often.
“We’re trying to do it as a last resort,” Storzillo said, “but a lot of these patients do require intubation.”
That means pumping air into and out of a set of lungs infected with an extremely contagious, potentially lethal pathogen.
“You have to take special precautions,” Storzillo said. “It’s a very high-risk procedure.”

Each intubation is conducted with the ambulance doors open and the vent fan on, should a patient cough despite the sedation.
Once the patient is intubated, a small HEPA filter is attached to the breathing bag, to trap the virus as the patient exhales.
On every call, Storzillo and Incorvaia don a so-called full-face respirator, which seals around the front of their head, protecting their eyes as well as their lungs. The respirators carry filters with a P100 rating from the National Institute of Occupational Safety and Health, better protection than the standard-issue N95 masks.
In addition to these protections, every single call is treated like a Covid-19 call.
While still on-scene, the paramedics wipe down each piece of equipment with a virucidal solution before packing it back in their truck. They then go “out-of-service,” bringing the truck back to the garage for further decontamination. All of their equipment is put in a decontamination tent —”decon” for short — and exposed to a sanitizing dose of ultraviolet light for at least 10 minutes. Only then can the truck be packed back up and dispatched on another call.
“There’s no way to be too clean,” Storzillo said. “Would I put this monitor on my mother or my grandmother? Absolutely not — not until it goes through the UV light and we decon it a couple times.”
So many are ‘dying at home’ these days

Paterson, a city of 146,000 people some 20 miles northwest of New York City, is statistically positioned to be hard hit by the pandemic.
Pitted against a disease that disproportionately affects both communities of color and those below the poverty line, the health care workers of Paterson have their work cut out for them. As of the last U.S. Census, 26% of Paterson’s population identified as black or African American, and 60% identified as Hispanic or Latino. Twenty-eight percent of the population reported being below the poverty line.
In Paterson, Storzillo said, “You have an incredibly diverse population and an incredibly underserved population.”

Storzillo spoke as he drove down Main Street, through a canyon of shuttered store front. Nonetheless, and despite the unseasonal chill, residents were out and walking around. Two men sat without masks on a bench in front of a 7-Eleven.
“You see people in this city that get sick from diseases that in more affluent areas — or middle-class areas, even — are completely managed,” Storzillo said. “You have people dying as a result of diabetes, you have people dying from seizures, because they either don’t have the access to medication or they don’t have the proper education from their physicians to take the medication as needed.”
“You see stuff here that you don’t see anywhere else,” he said. “People dying from asthma, severe, severe asthmatics, and it puts this population at an incredibly higher risk for Covid-19.”

As of Wednesday, 4,637 people in Paterson had tested positive for the disease, according to data released by the city. Of those, 148 have died.
Storzillo said he doubts those numbers tell the whole story.
“The amount of people that we’re pronouncing dead at home is astronomical,” he said. Before the outbreak, “we would maybe pronounce one or two people dead per shift, and they’d be elderly people on hospice that died of natural causes. Now we’re seeing 20-year-olds, 40-year-olds, that are all dying at home.”
“My fear is that they may not be counted in the numbers,” Storzillo said, estimating that some shifts had as many as eight deaths each since the coronavirus outbreak began. “It actually boggles my mind, the amount of people that we’ve been pronouncing outside of the hospital.”
The New Jersey Department of Health told CNN Tuesday that data on suspected Covid-19 home deaths was not available.
Citing “the overwhelming number of cases,” Donna Leusner, a spokesperson for the department, said that data on overall home deaths was also not available, although it will be later on.
A new dispatch code for a new time

Throughout the day, the word “pandemic” filled the air, most often in the crackly monotone of the dispatcher on the radio.
“They had to make a new dispatch code for ‘pandemic,'” Storzillo explained.
“‘Pandemic/exposure/outbreak,'” he said, echoing the official classification.

Now that the disease has become the paramedics’ new normal, however, the word is often simply appended on to more standard dispatch codes: “difficulty breathing — pandemic.”
But the distinction hardly matters.
“Every call, I’m wondering, is this the one where I could get it and then bring it home to my family?” Incorvaia said. His wife is a nurse in a nearby hospital. His children, ages 1 and 3, are cared for during the day by their grandparents.
Storzillo and Incorvaia both said they’ve agreed to treat every call as a pandemic call.
Last Wednesday, that meant a lot of fighting the wind while tying the straps on one another’s bright yellow protective gowns, checking fit on respirators, and doubling up on gloves, regardless of the dispatch code.
Volume’s down, but ‘it’s still so real’

Of the nine calls that Storzillo and Incorvaia answered on their shift, four were suspected Covid-19 cases. One man refused to go to the ER for unrelated diabetic issues, because of concerns over catching the virus. Four were “released to BLS” — taken to the emergency room by the “basic life support” EMTs — including two suspected Covid-19 patients who did not immediately require intervention by the paramedics.
For the past few weeks, the Paterson Fire Department’s EMTs have been supplemented by EMTs from elsewhere in the country, an arrangement brokered by the Federal Emergency Management Administration. The support has allowed the city’s EMTs to work less overtime, a bulwark against burnout.
There is no such arrangement in place for Paterson’s paramedics.
“There’s times when you’d have a shift, in years past, where you’ll have one or two sick people a shift, and you may have to intubate one of them,” Storzillo said. “Now in the past couple weeks we’ve been seeing three or four in a row where you have to intubate them … and they’re horrifically ill.”
“We’ve never had that before,” Storzillo said. “Dealing with all these patients one after another, it really wears on you.”
“Anybody who says they’re not scared during this is lying to you,” he added. “We may not feel it now, but, summer? Fall? when the dust settles, I think that a lot of first responders might be dealing with PTSD.”

For his part, Storzillo said that working with a friend helps. “He knows everything about me, and I think I know everything about him,” he said of Incorvaia. “Just the security of knowing that somebody has my back, I feel like I can get through this.”
Incorvaia agreed. “It’s reassuring. You know that you’re both watching each other’s back, and that no matter what happens there’s someone there to look out for you.”
But both men expressed concern that they’d be on this footing for a long time.
“We’re going to be dealing with pockets of Covid for the rest of the year,” Storzillo said. “I truly believe that. I can’t see us becoming completely lax — we’re always going to suspect it.”

“You don’t want to be the last person to catch Covid,” he added.
Incorvaia said he worried they’d be in this fight for a while.
“When we’re here driving through the city I’d say there’s a decent amount of people still on the sidewalks, not social distancing,” he said.
“The ER is still quite inundated,” Storzillo said. “Just today I went into the ER, and you get reminded of how serious this still is. You still see patients on ventilators. It’s almost like an eerie sort of quiet to what’s going on, all you hear is the hum of the ventilators.”
“Though our call volume’s been going down, you walk in there and it’s still so real,” he added.
A different kind of call, another intubation

At 6:01 p.m., the last call of the shift came in. The details were piecemeal: Traumatic injuries, a male of unknown age, head trauma, unconsciousness.
It was the kind of call that would have been typical two months ago.
Storzillo and Incorvaia got in their truck and sped across town. The dispatch computer led them to a furniture store, where a Paterson Fire Department ambulance was already outside. Storzillo and Incorvaia suited up in their protective gear as several EMTs and a fire supervisor walked out of the furniture store. They spoke, and went inside to see the patient.
“Makes no sense,” Storzillo said upon returning. He said the patient was bleeding from the nose and mouth, and had been found face down in a pool of congealed blood.
The man was wheeled out on a stretcher, and Incorvaia assisted the EMTs as Storzillo called ahead to the emergency room, then rushed back to the patient.
The back of the ambulance was a full house. The patient lay on the stretcher, his clothes cut off to search for wounds. Storzillo and Incorvaia were at opposite ends of the stretcher, along with two out-of-town EMTs. A needle was pushed through the man’s chest to relieve pressure on a suspected punctured lung. For the second time in three hours, the paramedics prepared for a field intubation.
This time, Storzillo crouched at the man’s head, looking down his throat with a small camera. Blood covered the man’s face and pooled around a cervical collar brace that had been placed around his neck. Copper-colored splotches of congealed blood marked the white hazmat suits of the EMTs.
“We have too much trauma in the airway,” Storzillo said to Incorvaia.
Incorvaia, near the man’s feet, was administering the drugs.
“How much ketamine?” he asked Storzillo, preparing the sedative.
“One hundred,” his partner responded.
Storzillo reached for a so-called rescue airway, a tool that goes down a patients’ throat and then inflates, clearing a path for the intubating tube through the man’s battered throat.
Bloodied tools on the floor, Storzillo completed the team’s second intubation of the day. The ambulance door was shut, and the team raced back across Paterson to the hospital.
“These calls,” Incorvaia would say later, “one minute you’re sitting there having your coffee, the next minute your adrenaline is pumping and some guy is almost dying in front of you.”

“With traumas,” he went on, “there’s nothing we can do, nothing in the field. You’ve got ten minutes — they need a surgeon. They need blood.”
The ambulance pulled into the ER bay, and the team prepared to move.
“Swap out the oxygen?” Incorvaia asked.
Storzillo grabbed at an oxygen bottle near the side door. Empty.
“This one is dead,” he said through his mask.
He grabbed at another. “This one is probably dead too.”
He turned, frustrated, to the out-of-town EMTs. “I know it’s Paterson, but–” he trailed off.
There was enough oxygen in the third tank. They wheeled the man from the ambulance, and through the doors of the emergency room.
New Jersey requires paramedics to check in on the status of their patients at the end of their shift.
Storzillo said later that he and Incorvaia will sometimes check on patients well after their legal obligation to do so has ended.
Storzillo said the last time he checked, a week after those calls, both the patients they intubated were still alive, but in poor shape. The man from the nursing home had been admitted to the intensive care unit with Covid-19. The head trauma patient had suffered a major stroke, then a fall.
A long day, and then another one

Back at the garage, Storzillo backed the truck in for the last time that day. It had been nearly 13 hours since the day began.
“Not only are we dealing with the Covid patients, we have everything else that’s happening,” he said. “It really wears on you. I feel completely wiped after a day like today.”
“Doing a 12-hour shift here during this pandemic?” he said. “You go home, you immediately want to shower and go to bed, and you have work the next day. You’ve got to be up at five in the morning and do it all over again.”
The two began the decontamination process again, and made notes on what medications needed to be replenished. The 7 p.m. to 7 a.m. crew had arrived.
The decontamination process began again. Together, the four paramedics replenished the medications used over two intubations and seven other calls.
The sun was beginning to set, and the work was about to begin again.













{kind=link}